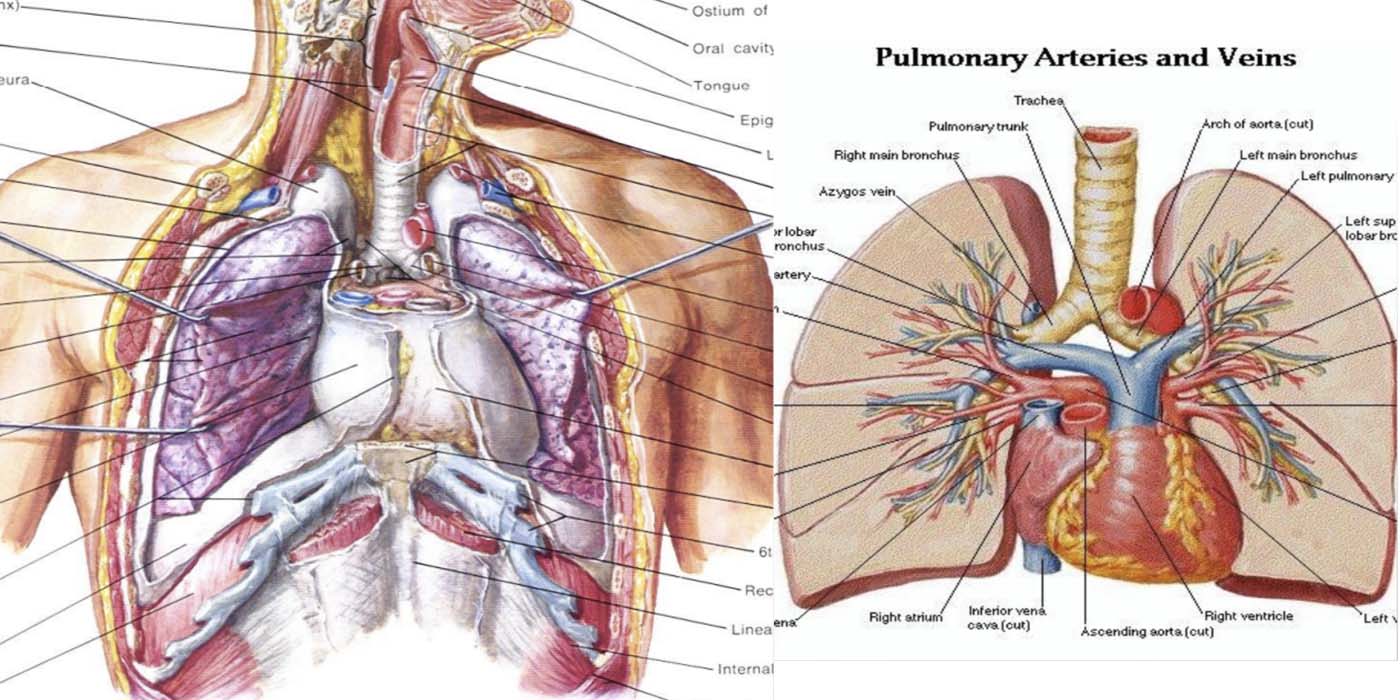
Anatomy
The lungs are a pair of organs in the chest whose primary function is for breathing.
The linings of the lungs are called pleura. On each breath, the diaphragm is contracted and creates a negative pressure in the thoracic space and air is drawn into the lungs, where gas exchange occurs. Deoxygenated blood is brought to the lungs by the pump action of the right ventricle, upon which oxygenation occurs. Oxygenated blood is then returned to the left atrium and subsequently to the left ventricle of the heart, which then pumps to the rest of the body.
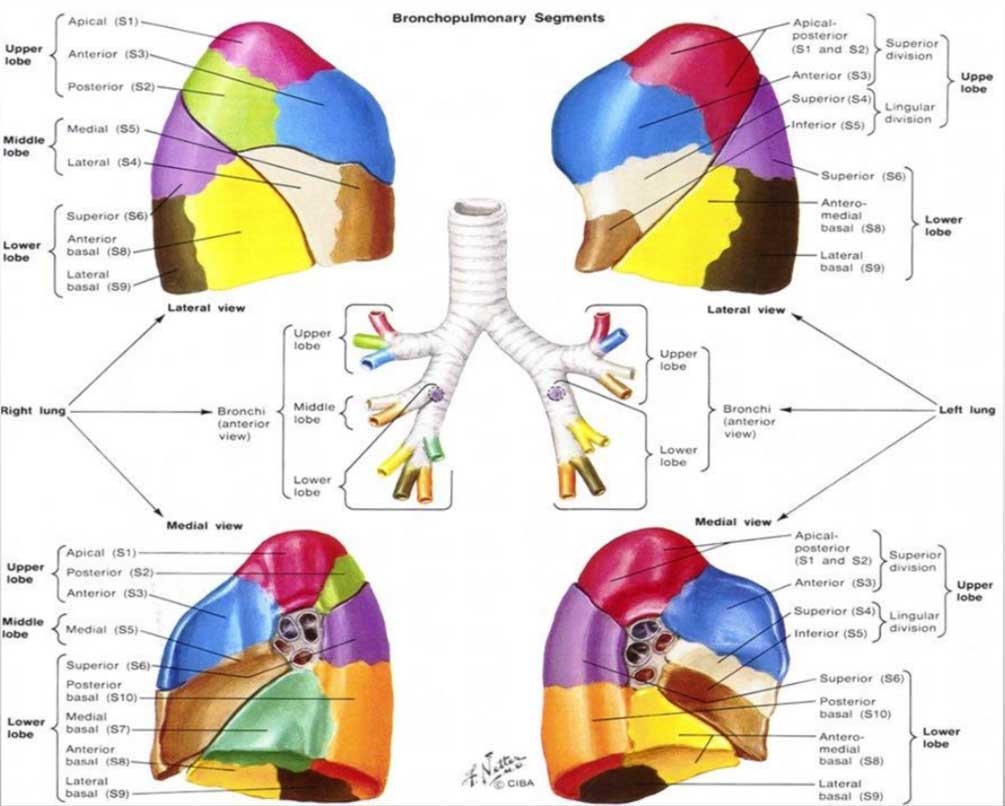
The lungs are made of smaller parts called lobes. The right lung has three lobes (upper, middle and lower lobes), whilst the left lung has two (upper and lower lobes). Each lobe can be divided again into smaller subsections called segments. The right side has 10 segments and the left side has 9 segments, as shown in the diagram below.
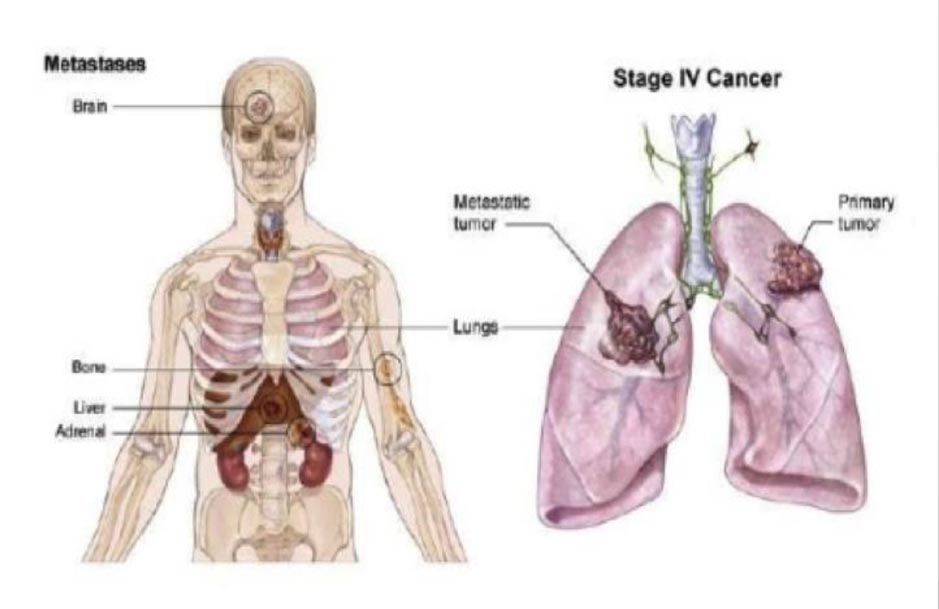
Lung cancers can be divided into primary lung cancers (originating from the lung) or secondary lung cancers (originating from other organs and metastasized to the lungs).
Primary Lung Cancer
Primary lung cancers are divided into two types. Small cell lung cancers comprise 15% of such primary lung cancers, while non-small cell lung cancers comprise 85%.
Small cell lung cancers are mostly centrally located near the main airways, making surgery impossible. In this case, the mainstay of treatment is chemotherapy and/or radiotherapy.
Non-small cell lung cancers (NSCLC) are more peripherally located within the lung and are more amenable to surgical treatment.
Non-small cell lung cancer (85%)

Small cell lung cancer (15%)
Symptoms of lung cancer
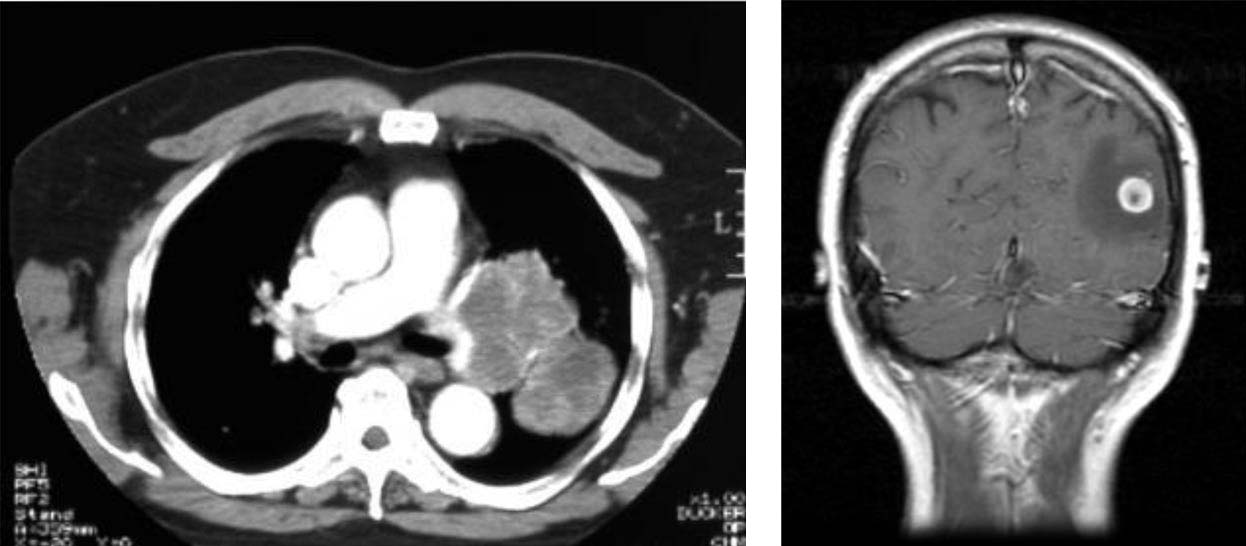
Symptoms of lung cancer depend on location and size of the tumour. Primary tumours may cause cough, hemoptysis, chest pains and shortness of breath. Larger tumours may invade local structures like the superior vena cava, resulting in swelling of the face (SVC syndrome), of vocal cords (hoarseness of voice), or of the oesophagus (resulting in difficulty swallowing). If the tumour has metastasised, patients may then experience bone pain, headaches and lymph node enlargements. Systemic symptoms may be weight loss and poor appetite.
There is no accepted mass screening method for lung cancer.
Chest x-ray (CXR), blood tumour markers, sputum cytology have poor yields.
A low dose CT scan is the best method for screening. It has 5 times less radiation than conventional CT, and is equivalent to undergoing 15 CXRs. It is very sensitive and is able to detect even the tiniest nodules in lungs.
For those using a CT coronary angiogram to screen for heart disease, lung nodules may be detected incidentally as well.
It is recommended for a person to screen for lung cancers if you are a smoker or an ex-smoker over 55 years of age, if you have a family history of cancers, or a previous history of cancers.
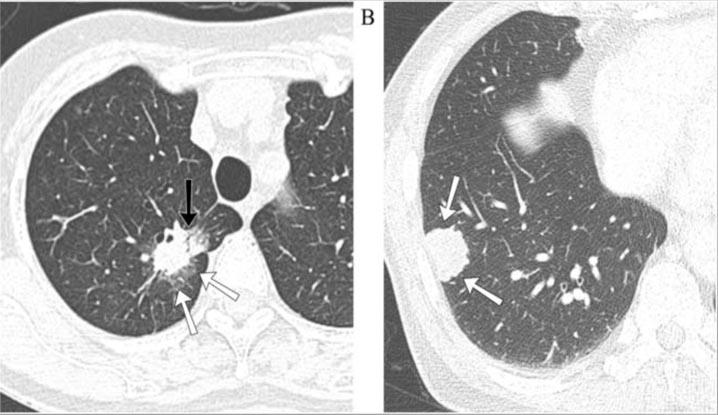
Ground Glass Opacities
CT lung screenings frequently report the presence of ground glass opacities (GGO) in the lungs. These are grey patches in the lung. They are non-solid areas of lungs which may be cancer, inflammation or infection. These need to be examined by a lung specialist, who may suggest watching the lesion closely by repeating the CT scan every 6 months. By watching closely, if the lesion persists, enlarges or develops solid components, then it is very likely that the GGO is an early cancer. Another suggested option is surgical removal of the lesions.

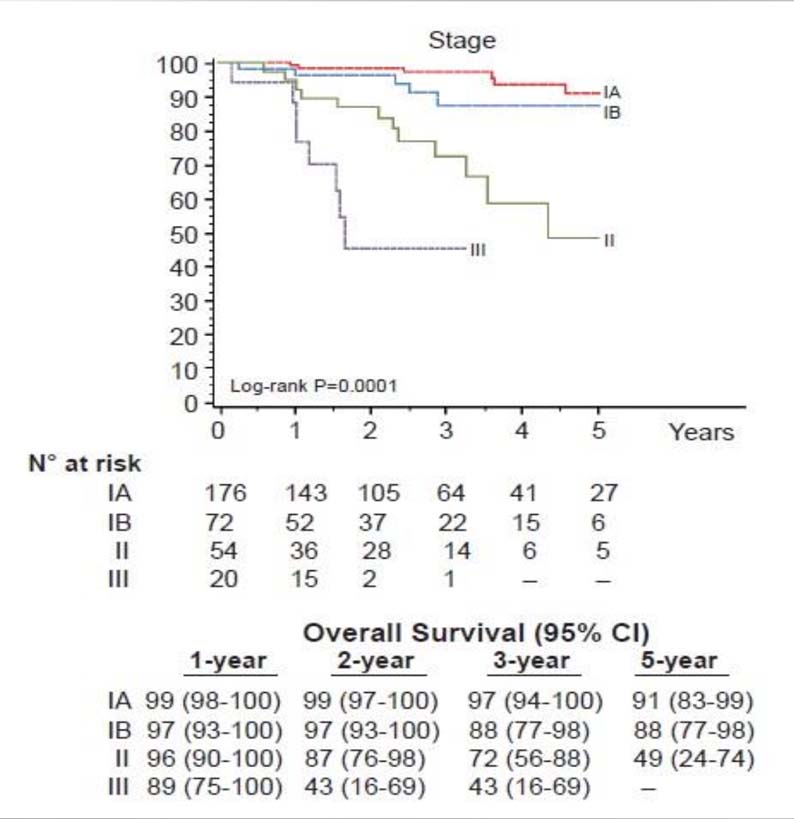
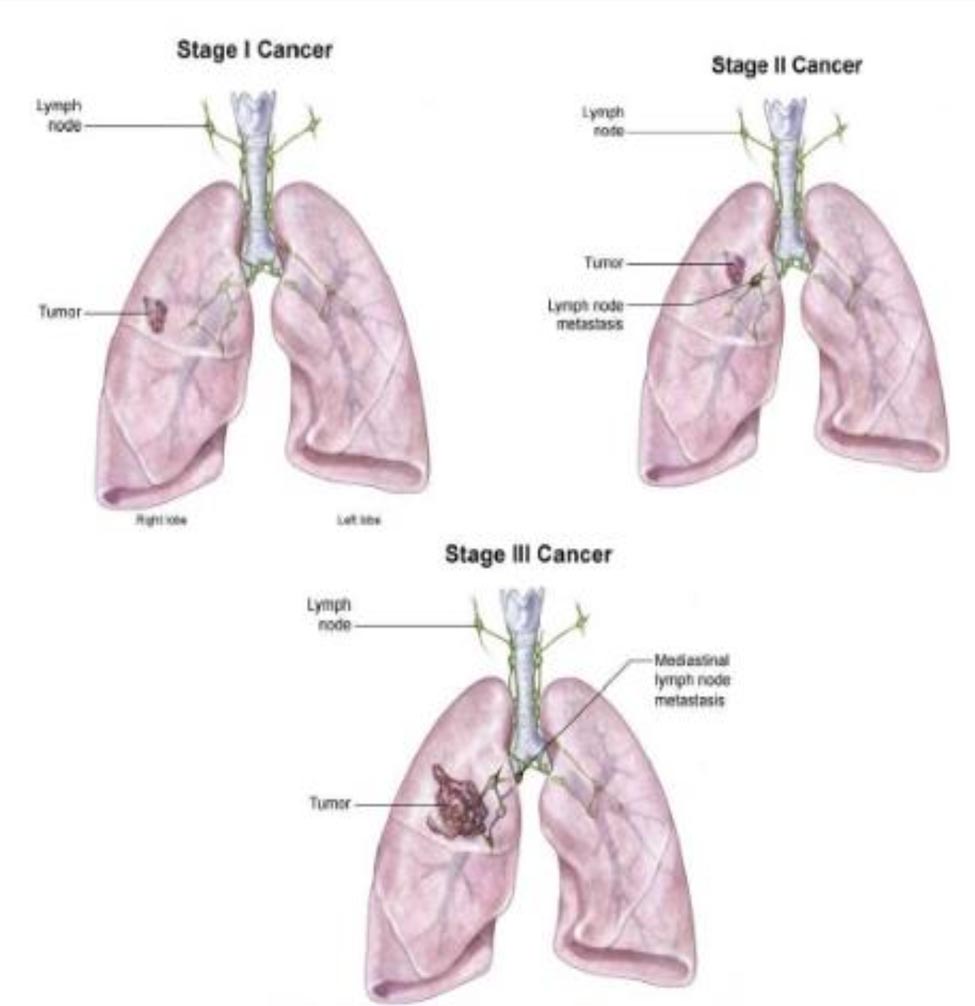
Stages of Lung Cancer
Lung cancer can be divided into 4 stages determined by the size of the primary tumour, presence of lymph nodes and whether there is metastasis to the rest of the body. Prognosis for long term survival is related to the stage of lung cancer determined when the patient first presents symptoms, as shown in the survival chart below.
STAGE I
No lymph node involvement
STAGE II
Lymph nodes involved, or tumour invading into chest wall
STAGE III
Mediastinal nodal involvement or bad tumour factors
STAGE IV
Metastatic disease